The abdomen and pelvis are usually studied initially by sonography because it is less expensive, widely available, and does not use ionizing radiation. Subsequently and depending on the particular clinical application, CT scans are obtained when it is necessary to clarify sonogram findings.
However, for certain applications, CT scans are obtained upfront instead of after sonograms.
For the evaluation of female pelvic reproductive organs, MRI scans, not CT scans, are obtained after sonography because they obtain essential detail superior to CT scans and without the use of ionizing radiation. For the staging of early prostate cancer, MRI is superior to CT to determine if the tumor has just spread outside the prostate capsule so it can be obtained instead of a CT scan.
In the abdomen, MRI is usually used to clarify findings from a CT scan or when the CT scan is negative and pathology is still suspected. MRI also allows for dedicated studies of solid organs using dynamic techniques in which multiple scans of the liver and/or pancreas are obtained without exposing the patient to ionizing radiation. There are several types of intravenous contrast dedicated to the liver that increase the specificity of the nature of liver lesions detected by CT and sonography. These contrast media also increase sensitivity by allowing detection of lesions that are not detectable by CT and sonography usually due to their small size.
MRI allows the evaluation of the pancreatic duct and bile ducts inside and outside the liver by MRCP (magnetic resonance cholangiopancreatography).
Image 1
Abdominal sonogram. Gallbladder stones. Sonography is the most sensitive modality to establish this diagnosis
Image 2
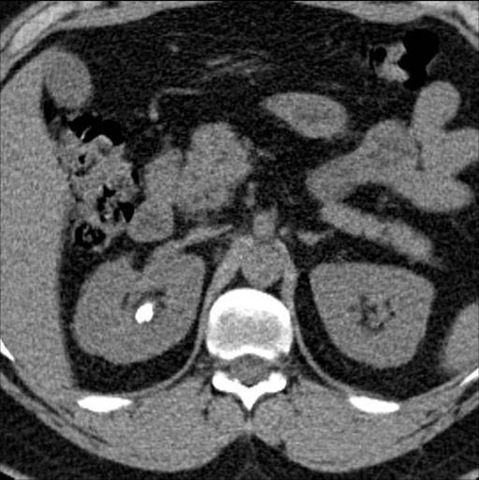
Abdominal CT without intravenous contrast. White focus on right kidney represents a stone
Image 3
Pelvic CT without intravenous contrast. White focus represents stone stuck in the insertion of the ureter into the bladder. Patient with a lot of pain on his right side
Image 4
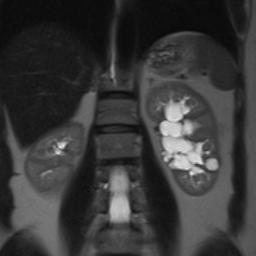
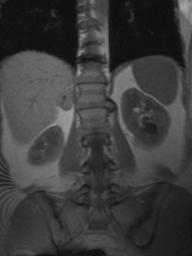
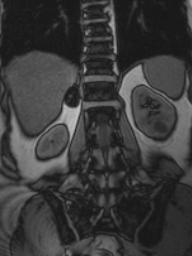
MRI abdomen. Sonogram and anterior abdominal CT suggest hydronephrosis on the left side. MRI shows bright confluent areas deep in the left kidney
Image 5
Same patient as Imaging 4 after injecting intravenous gadolinium contrast. No obstruction/hydronephrosis. The worrisome finding in previous studies represents a collection of parapelvic cysts simulating hydronephrosis
Image 6
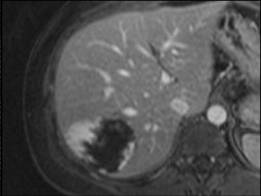
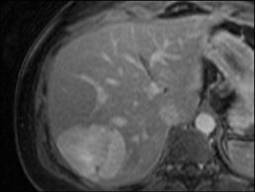
Abdominal MRI using dynamic protocol to evaluate liver mass, early arterial phase. Mass captures gadolinium in its periphery
Image 7
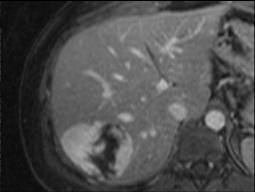
Abdominal MRI using dynamic protocol, portal venous phase. The gadolinium has progressed to the center in the liver mass
Image 8
Abdominal MRI using dynamic protocol, late phase. The gadolinium in the mass has progressed to completely fill the liver mass. Enhancement pattern is typical for hemangioma. Not all hemangiomas demonstrate this pattern of intravenous contrast uptake but when it occurs, it is classic for this diagnosis. Other images obtained in all MRIs are used routinely
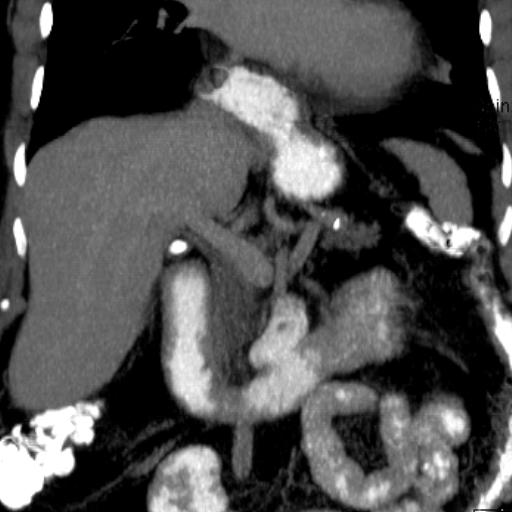
Image 9
Intravenous non-contrast abdominal CT scan in a patient with lung cancer demonstrates a mass in the right adrenal gland between the liver, inferior vena cava and the right diaphragm. Lung cancer has a propensity to spread to the adrenal glands. A patient with allergies to iodine-based intravenous contrast and wanting to avoid additional radiation by CT. An abdominal MRI using chemical shift imaging sequences is recommended. MRI is more specific than CT for certain diagnoses of adrenal masses such as lipid-rich adenomas and pheochromocytomas.
Image 10
Abdominal MRI, in phase image, shows the mass in the right adrenal gland that was seen on the CT scan (image 8)
Image 11
Abdominal MRI, out of phase image, shows the mass in the right adrenal gland that was of intermediate sign becomes completely black (hypointense). MRI is more specific than CT to establish whether an adrenal mass contains microscopic fat as is the case here. The findings are typical for an adenoma rich in adrenal lipids reliably ruling out metastatic disease
Image 12
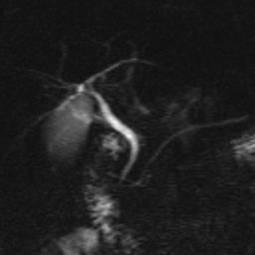
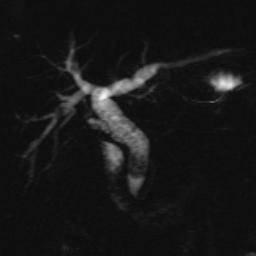
MRCP (magnetic resonance cholangiopancreatography) is a non-invasive alternative to endoscopic cholangiopancreatography performed by the gastroenterologist or surgeon. MRCP is often performed as a guide prior to the endoscopic version to increase the likelihood of success in cases where an intervention is required. The study visualizes the bile tree inside and outside the liver and gallbladder and does not require intravenous contrast or ionizing radiation. This image demonstrates an anatomical variant called pancreas divisum. People with this variant are prone to developing pancreatitis
Image 13
MRCP. Diffusely dilated bile ducts inside and outside the liver. A large stone is visualized in the common bile duct obstructing the drainage of bile produced in the liver responsible for the dilation of the biliary tree
Image 14
Pelvic CT with intravenous contrast. Left side of the uterus irregular. The image without intravenous contrast (not included) showed no calcifications in the uterus. Although sonography is an alternative at this time, the patient had an MRI of her pelvis to obtain the best possible anatomical detail and to study the possibility of masses surrounding the endometrial cavity
Image 15
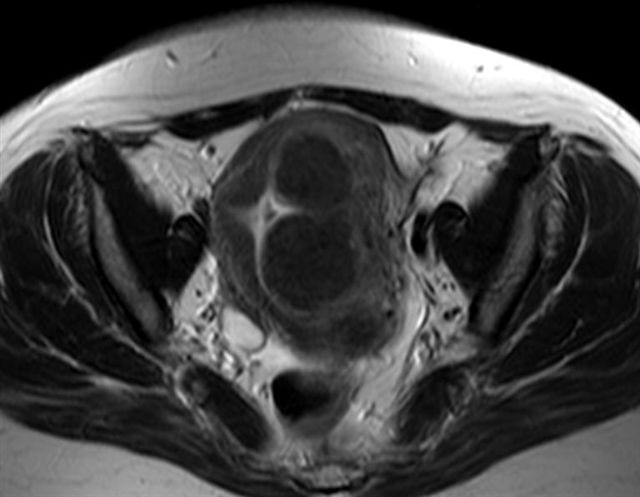
MRI pelvis from the same patient from image 14 shows that the area of concern on CT represents a series of dark masses that involve both the muscle of the uterus (myometrium) and the endometrial cavity. The appearance is classic of fibroids (leiomyomas), the most common uterine tumor, typically benign
Image 16
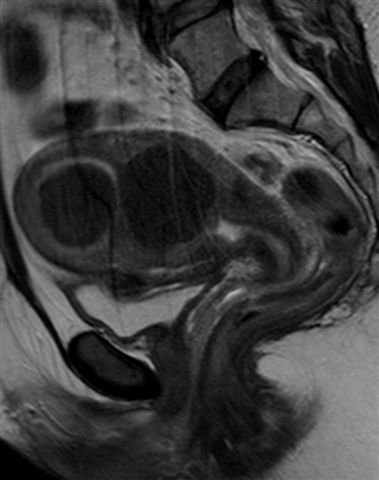
Pelvic MRI showing fibroids from sagittal/lateral perspective. The image reveals that there is another small superficial fibroid making contact with the upper part of the urinary bladder
Image 17
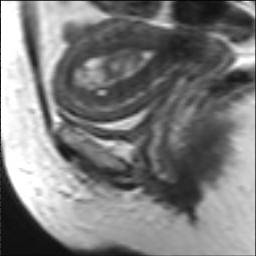
MRI pelvis. Thickened and heterogeneous endometrium due to primary cancer. No evidence of invasion of the muscle of the uterus (myometrium)
Would you like to schedule an appointment?
Now you can make appointments online with San Patricio MEDFLIX.