Arteries are studied more often than veins.
CTA represents the non-invasive version of a catheterization obtained in a computerized tomography (CT) machine. MRA represents the non-invasive version of a catheterization obtained on a magnetic resonance imaging (MRI) machine. The “A” in the abbreviations CTA and MRA stands for “angiography.
By definition, all CTA studies require the injection of intravenous contrast. While in the past, all MRA studies were performed without intravenous contrast, technological advances have changed the technique so that today all MRAs, except those performed on the brain, routinely require the injection of intravenous contrast. For some particular indications, brain MRA is performed with the injection of intravenous contrast.
The benefits of performing an angiographic study in one modality over another are the same as they would apply to any part of the body. While a CTA is less expensive than an MRA, CTA requires ionizing radiation and requires iodine-based intravenous contrast that is potentially nephrotoxic. MRA does not use ionizing radiation; it uses magnetic fields and radiofrequency pulses. MRA intravenous contrast is gadolinium-based, not iodine-based, and is not nephrotoxic. However, in patients who already have compromised kidney function (defined as a glomerular filtration rate of 30 or less ml/min/1.73 m2 ), it is recommended that gadolinium-based intravenous contrast for MRA not be used. These same patients with compromised renal function usually also do not inject iodine-based contrast for CTA unless a dialysis session is planned, not because of risk to the kidneys since in that scenario the kidneys are already very compromised, but to avoid other problems related to intravascular volume.
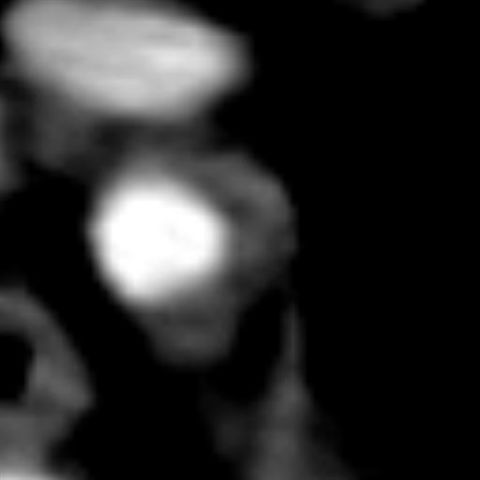
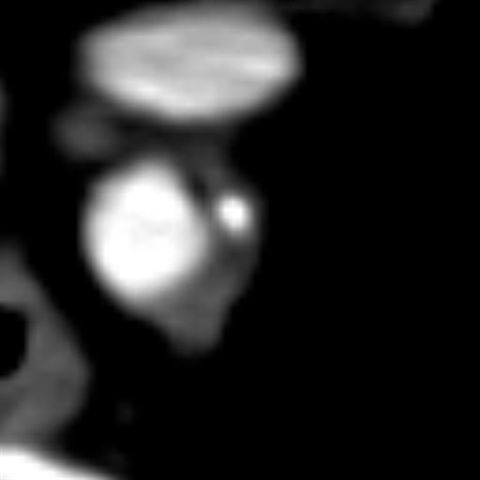
Apart from these factors mentioned above, during the evaluation of atherosclerotic disease CTA can differentiate between calcified and non-calcified plaques. See image 1, non-calcified (gray) plaque from an artery in the upper center of the chest called the mediastinum and see image 2, calcified (white) plaque in the same artery.
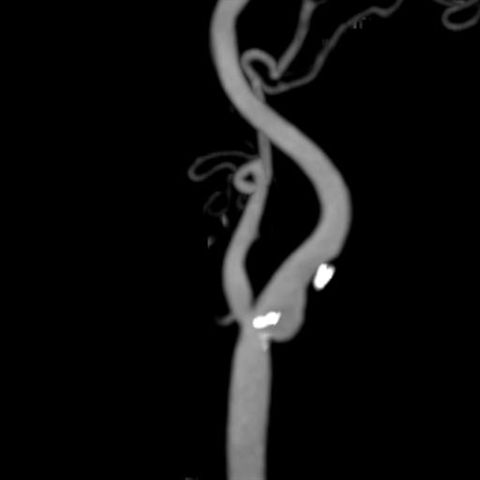
MRA cannot currently visualize calcified plaques. See Images 3 and 4, normal and abnormal MRA respectively of the carotid arteries in the neck. There is severe disease on Image 4, but the obstructive plaque cannot be discerned, only disease can be inferred due to the greatly reduced calcification of the carotid artery. Images 5 and 6 are from a neck CTA showing calcified (white) plaques displayed in color and gray scale respectively that reduce the caliber of the internal carotid bulb. Unlike the MRA in Image 4 which demonstrates disease but cannot visualize the plaques.
Image 7 of an MRA of the aortic callus in the chest routinely obtained as part of every neck MRA shows that no plaque can be discerned. The same patient had a CTA from the same anatomical region, see Image 8, routinely obtained as part of every neck CTA, which shows that the patient has atherosclerotic disease, evident by calcified (white) plaques. Prominent atherosclerotic plaques may be present, sometimes without producing any obstruction, especially in the early stages so that MRA may give negative results when the disease may be present (false negative).
Particular situations, heart arteries and leg arteries.