At present, CTA is superior and preferred over MRA for studying the arteries of the heart. The CT scanner to be used to properly study the coronary arteries must be no less than 64 detector rows (available from all major CT companies) or two-tube x-ray equipment (currently only available from some Siemens company models). Otherwise, the results obtained will not be sufficiently reliable as stated in the most recent literature. For the Medicare patient population and major PR plans, this study has to be performed on equipment that has such technical requirements.
Another relevant fact is that the radiologist or other specialist who supervises and prepares protocols for the optimal performance and interpretation of these studies must have special additional credentials documenting proficiency in performing and interpreting these complex CTA scans.
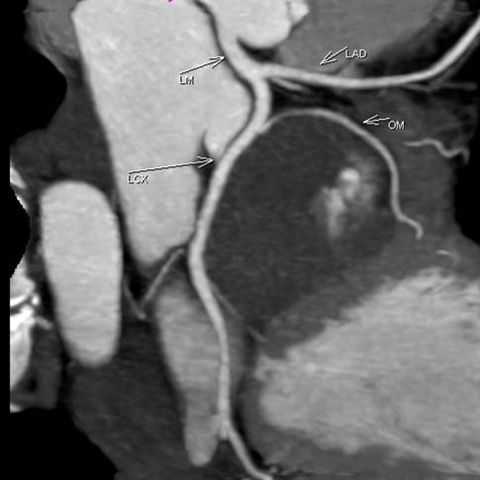
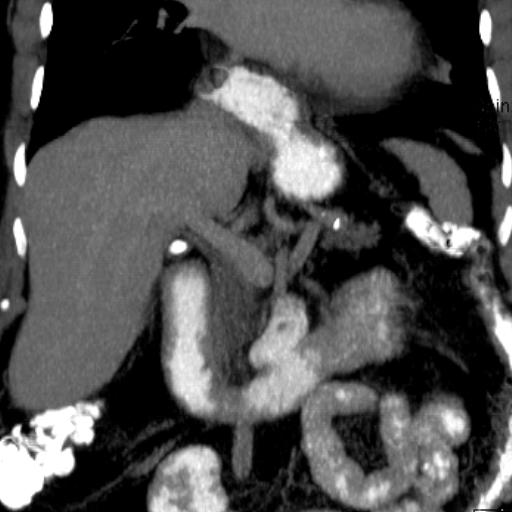
Most coronary CTA studies begin with a coronary calcium scoring study before the intravenous contrast is injected (see Figure 9). This part of the study, which can also be performed independently of coronary CTA, detects and quantifies the volume of calcified plaques present in each major coronary artery and generates a score. This score is highly correlated with the probability that the person will experience an adverse cardiac event within the next few years. If the score is too high, the recommendation is that intravenous contrast should not be injected and the patient should go directly for coronary catheterization. At present, too much calcium in the arteries precludes optimal evaluation of the coronary arteries. Coronary calcium scoring does not detect non-calcified plaque. In order to detect this type of plaque, which is usually responsible for heart attacks, it is necessary to complete the study by injecting intravenous contrast. As in the examples of the neck arteries in the previous section, the coronary CTA study can distinguish between noncalcified plaques and calcified plaques (see Image 10, first arrow delineating noncalcified plaque and second arrow calcified plaque).
Coronary CTA requires intense work and processing at a workstation to generate a diversity of images, among which are impressive in multiplanar format, cinematic and isolated from the rest of the heart muscle. See images 11 and 12. Image 13 demonstrates the relationship of the coronary arteries near their origin in reference to a pericardial mass (the cover of the sac within which the heart is located).

Image 1
Coronary Calcium Scoring, Left anterior descending coronary artery
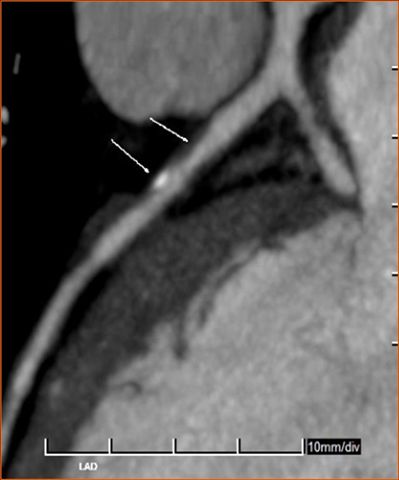
Image 2
Coronary CTA, noncalcified and calcified plaques
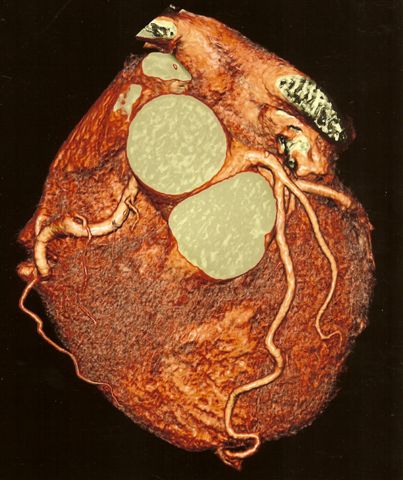
Image 3
Coronary CTA, color shaded volume rendering
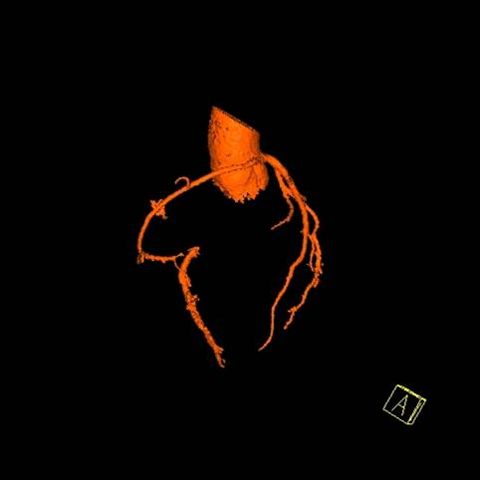
Image 4
Coronary CTA isolating coronary arteries at aortic origin