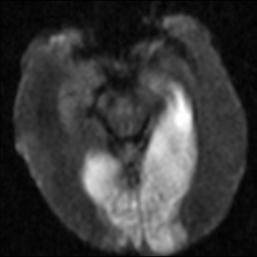
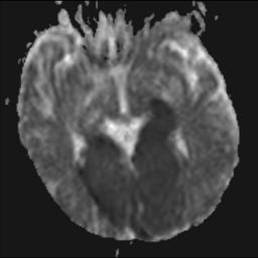
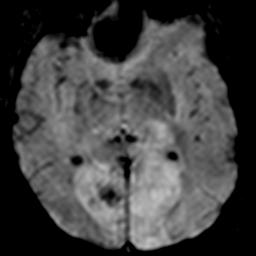
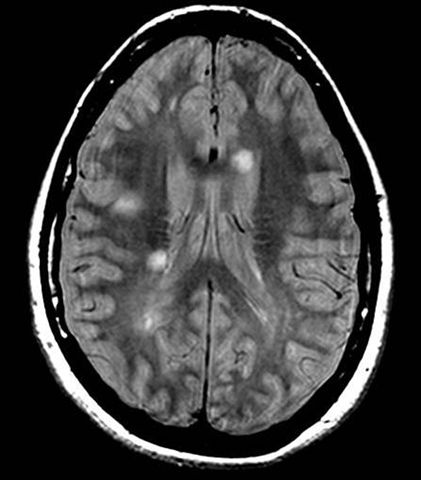
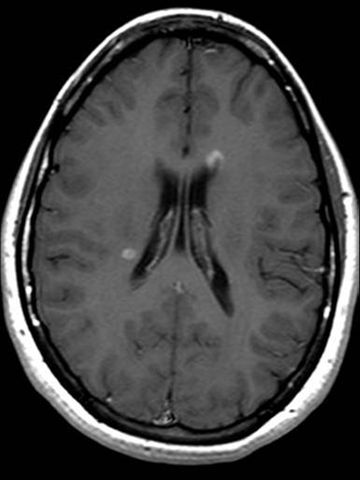
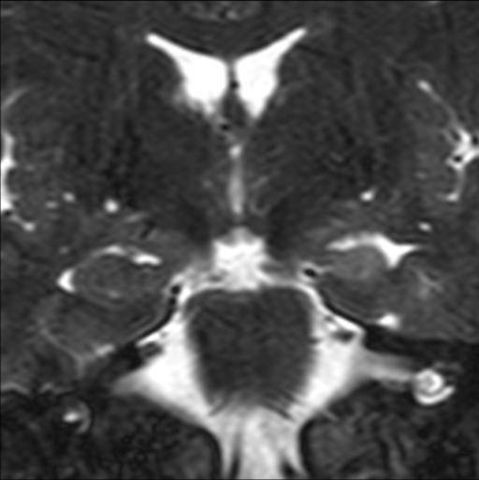
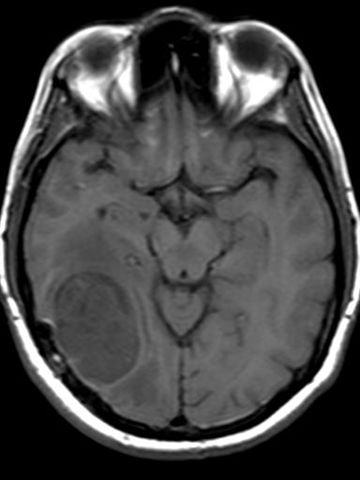
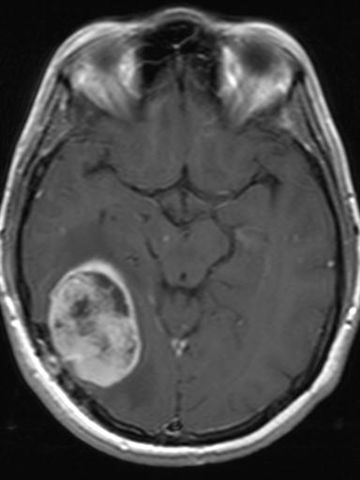
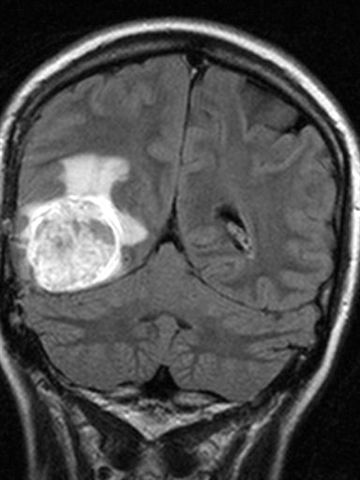
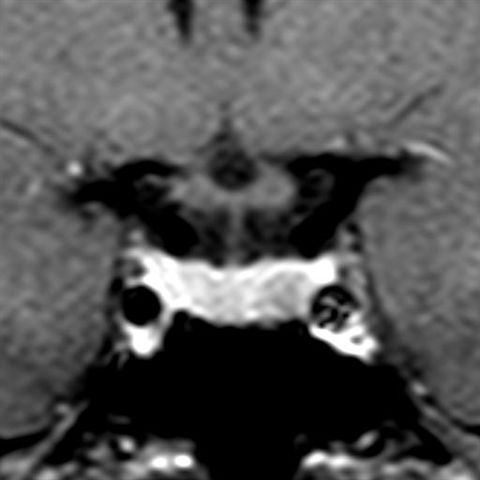
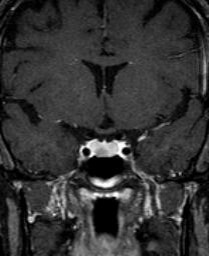
Neuroradiological anatomical studies include the brain, the spine, and the anatomy attended to by the otolaryngologist. For brain studies, for the vast majority of indications, MRI is the study of choice, although more expensive than CT. However, the CT scan, although using ionizing radiation, continues to be more available and the first line study particularly in emergency rooms and in the clinical setting of trauma, suspected subarachnoid and subdural hemorrhage and suspected recent cerebral infarction. When head trauma is suspected, negative calvarium radiographs do not rule out fracture, much less brain damage. To evaluate hyperacute cerebral infarction (images 3, 4 and 5), white matter disease (multiple sclerosis, vasculitis, among many others; images 6 and 7), cranial nerves (image 10), masses (images 13, 14 and 15), the pituitary gland (image 16), the pineal gland, among many other indications, MRI is the study par excellence, often requiring intravenous gadolinium contrast.
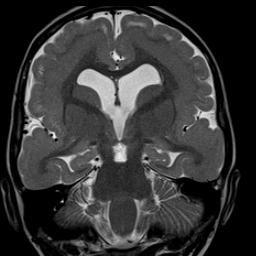
The definitive evaluation of the sinuses and the temporal/mastoid bones and bone labyrinth is performed with CT. MRI without and with intravenous gadolinium complements both studies, most frequently the temporal bones when seeking to distinguish recurrent cholesteatoma from scar tissue and for the evaluation of the membranous labyrinth and the nerves of the internal auditory canals. The evaluation of cerebral dysgenesis is performed with wide superiority with MRI over CT (image 12).
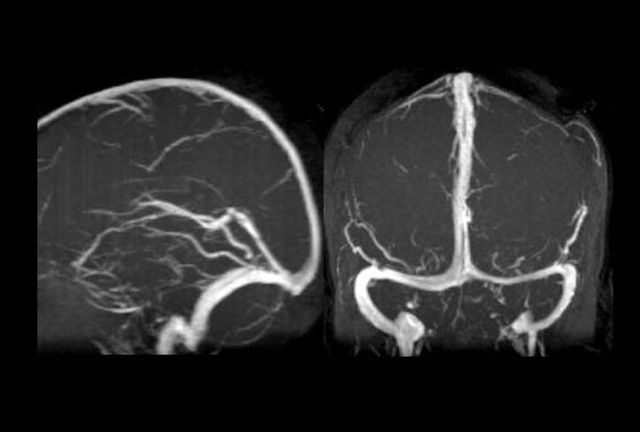
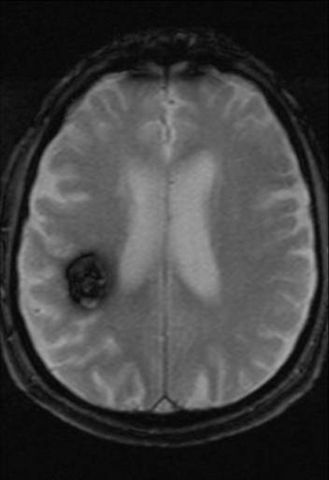
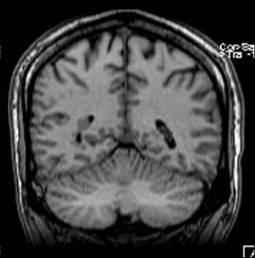
The evaluation of cerebral vascular malformations (image 9) is performed by MRI without and with gadolinium. The evaluation of cerebral aneurysms is performed by MRA or CTA. Please refer to the previous section that outlines these non-invasive modalities to study the blood vessels. The best evaluation of the venous dural sinuses in the brain is done by the combination of MRI without and with gadolinium and MRV (see image 1).
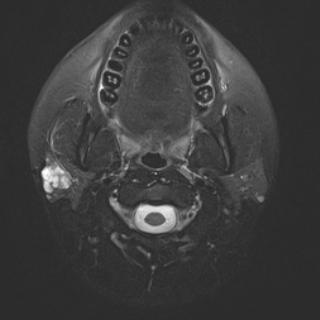
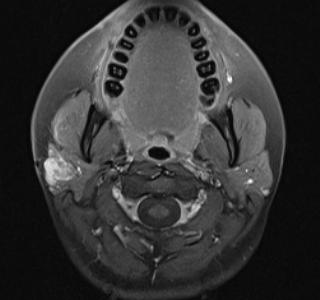
Evaluation for most neck and orbit indications is optimally performed with neck MRI and orbit MRI respectively, both without and with gadolinium. Some indications such as stone detection in the salivary glands and ducts are best performed with CT.
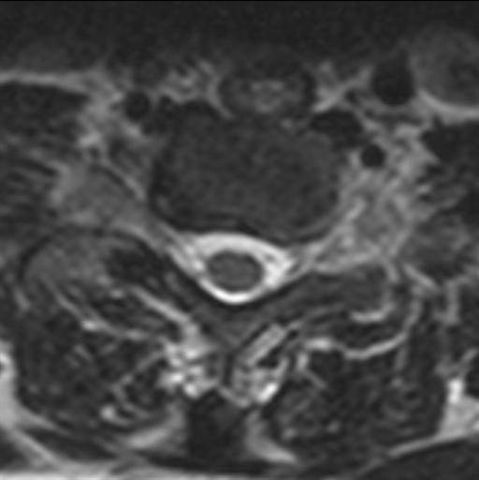
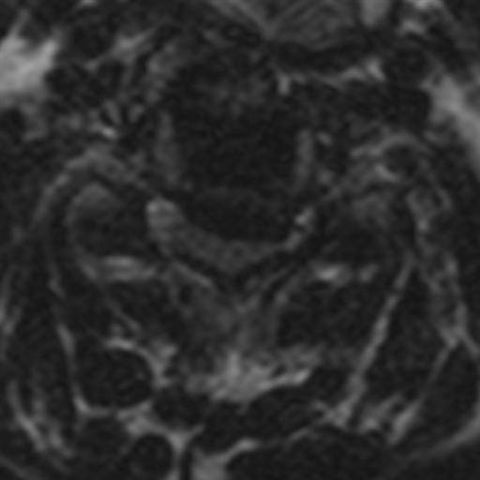
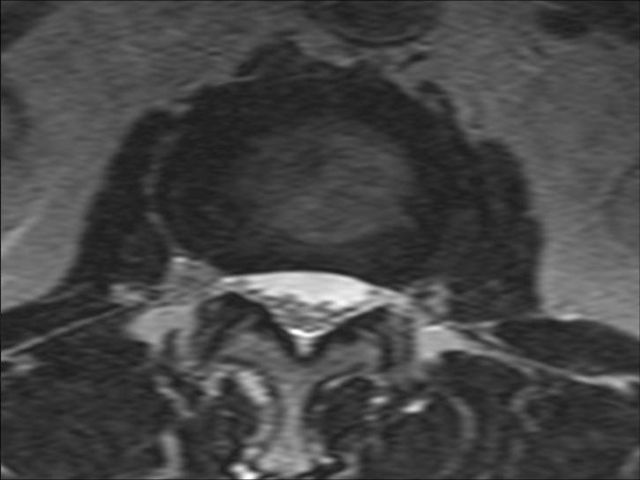
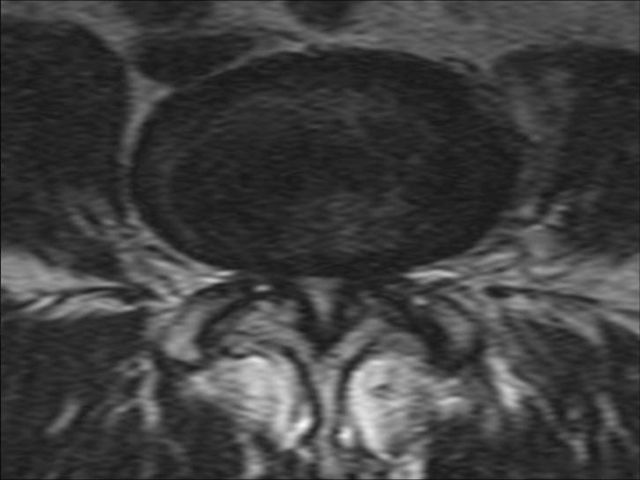
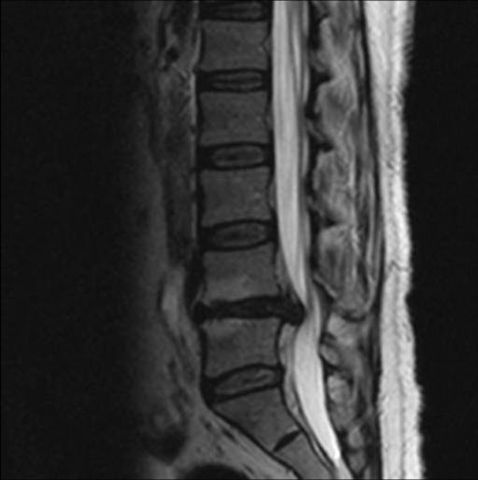
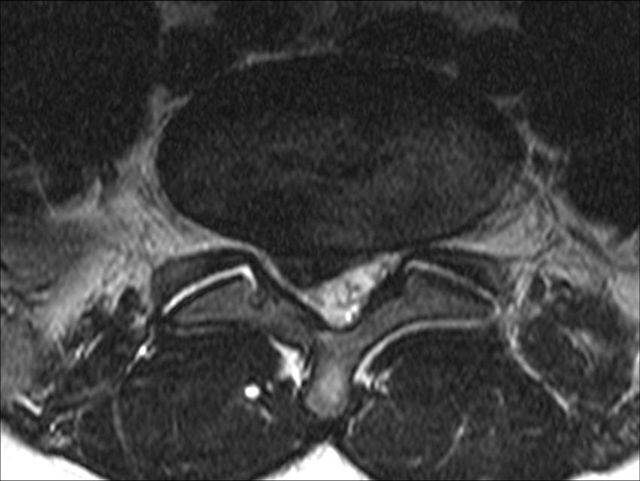
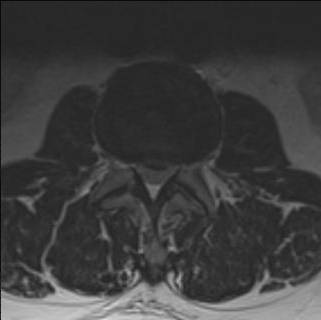
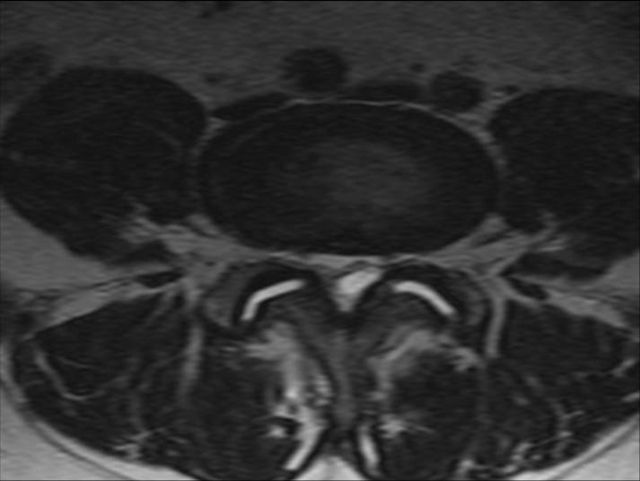
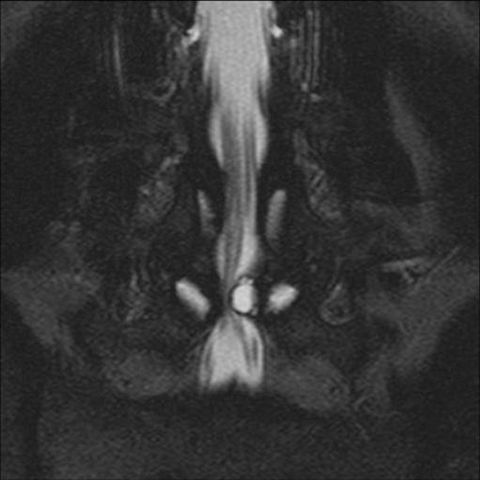
The spine is studied by segments to achieve sufficient detail so that for both CT and MRI, studies of the cervical, thoracic and lumbosacral spine represent separate anatomical regions. MRI, in addition to not using ionizing radiation, demonstrates the presence of herniated discs and various masses in a consistent and reliable manner. CT scans of these regions of the spine do not allow evaluation of discs in some segments and do not allow differentiation between recurrent herniated and scarred discs in the normal spine. MRI is superior during the evaluation of disc infection and adjacent vertebrae and for most cases of metastatic disease.